|
Overview
 Morton's neuroma is named after Dr Morton who first described this condition in 1876. It is sometimes called Morton's metatarsalgia or interdigital neuroma. It is a condition that affects one of the common plantar digital nerves that run between the long bones (metatarsals) in the foot. It most commonly affects the nerve between the third and fourth metatarsal bones, causing pain and numbness in the third and fourth toes. It can also affect the nerve between the second and third metatarsal bones, causing symptoms in the second and third toes. Morton's neuroma rarely affects the nerve between the first and second, or between the fourth and fifth, metatarsal bones. It tends to affect only one foot. It is rare to get two neuromas at the same time in the same foot. Morton's neuroma is named after Dr Morton who first described this condition in 1876. It is sometimes called Morton's metatarsalgia or interdigital neuroma. It is a condition that affects one of the common plantar digital nerves that run between the long bones (metatarsals) in the foot. It most commonly affects the nerve between the third and fourth metatarsal bones, causing pain and numbness in the third and fourth toes. It can also affect the nerve between the second and third metatarsal bones, causing symptoms in the second and third toes. Morton's neuroma rarely affects the nerve between the first and second, or between the fourth and fifth, metatarsal bones. It tends to affect only one foot. It is rare to get two neuromas at the same time in the same foot.Causes Some experts believe that other foot conditions may also be associated with Morton's neuroma. This is because other conditions may cause the metatarsal bones to rub against the nerve in your foot. Foot problems that may increase your risk of developing Morton's neuroma include abnormally positioned toes, high arches, where the arch or instep of your foot is raised more than normal, flat feet, low arches or no arches at all, bunions a bony swelling at the base of the toe. Hammer toe, where the toe is bent at the middle joint. Being active and playing sport can make the painful symptoms of Morton's neuroma worse. In particular, running or sports that involve running, such as racquet sports, can place extra pressure on the nerve in your foot, which can aggravate the problem. Symptoms A Morton's neuroma causes a "burning" sharp pain and numbness on the bottom of the foot in the involved area, and this pain and numbness can radiate to the nearby toes. The pain is usually increased by walking or when the ball of the foot is squeezed together and decreased with massaging. It may force a person to stop walking or to limp from the pain. Diagnosis The most common condition misdiagnosed as Morton's neuroma is metatarsophalangeal (MTP) joint synovitis. When pain occurs in the third interspace, the clinician may misdiagnose the condition as Morton's neuroma instead of MTP synovitis, which may manifest very much like Morton's neuroma. MTP synovitis is distinguished from Morton's neuroma by subtle swelling around the joint, pain localized mainly within the joint, and pain with forced toe flexion. Palpation of the MTP joint is performed best with a pinching maneuver from the dorsal and plantar aspects of the joint to elicit tenderness of the joint. Other conditions often misdiagnosed as Morton's neuroma include the following. Stress fracture of the neck of the metatarsal. Rheumatoid arthritis and other systemic arthritic conditions. Hammertoe. Metatarsalgia (ie, plantar tenderness over the metatarsal head) Less common conditions that have overlapping symptoms with Morton's neuroma include the following. Neoplasms. Metatarsal head osteonecrosis. Freiburg. steochondrosis. Ganglion cysts. Intermetatarsal bursal fluid collections. True neuromas. Non Surgical Treatment Common treatments involve wearing different shoes or using arch supports. Resting the foot, massaging the toes and using an ice pack may work for some people. A GP or a podiatrist (foot specialist) may also recommend anti-inflammatory painkillers or a course of steroid injections. Numbing injections, in which alcohol and a local anaesthetic are injected into the affected area of the foot, may also be effective. In extreme cases, when the condition does not respond to treatment, day case surgery may be needed.  Surgical Treatment If symptoms do not respond to any of the above measures then surgery may be suggested. This involves a short 30 minute operation to either remove tissue to take pressure off the nerve or to remove the nerve causing the pain. The surgery can be done as a day case but it will be two or three weeks before you can be fully active on your feet. There may be some lingering numbness afterwards if the nerve is removed. But surgery is successful in around 80% of cases. There is a small risk of complications such as infection and thickening of the skin on the soles of the feet. There are actually two unique variations of leg length discrepancies, congenital and acquired. Congenital indicates you are born with it. One leg is structurally shorter compared to the other. As a result of developmental periods of aging, the brain picks up on the stride pattern and recognizes some variation. Your body typically adapts by dipping one shoulder over to the "short" side. A difference of less than a quarter inch is not grossly excessive, doesn't need Shoe Lifts to compensate and generally won't have a serious effect over a lifetime.
 Leg length inequality goes largely undiagnosed on a daily basis, however this problem is easily fixed, and can eradicate numerous cases of back discomfort. Therapy for leg length inequality usually involves Shoe Lifts. These are typically economical, in most cases being less than twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Mid back pain is the most prevalent ailment impacting men and women today. Around 80 million men and women experience back pain at some stage in their life. It is a problem that costs businesses millions of dollars each year due to lost time and productivity. Innovative and better treatment solutions are constantly sought after in the hope of decreasing the economic influence this condition causes.  Men and women from all corners of the world suffer from foot ache due to leg length discrepancy. In these cases Shoe Lifts can be of immense help. The lifts are capable of reducing any discomfort in the feet. Shoe Lifts are recommended by many specialist orthopaedic orthopedists. So that you can support the human body in a nicely balanced manner, the feet have a crucial role to play. In spite of that, it is often the most neglected region in the human body. Many people have flat-feet which means there is unequal force exerted on the feet. This causes other parts of the body including knees, ankles and backs to be affected too. Shoe Lifts make sure that ideal posture and balance are restored.  Overview OverviewHammer, claw, and mallet toes are toes that do not have the right shape. They may look odd or may hurt, or both. Tight shoes are the most common cause of these toe problems. A Hammertoes is a toe that bends down toward the floor at the middle toe joint. It usually happens in the second toe. This causes the middle toe joint to rise up. Hammer toes often occur with bunions. Claw toe often happens in the four smaller toes at the same time. The toes bend up at the joints where the toes and the foot meet. They bend down at both the middle joints and at the joints nearest the tip of the toes. This causes the toes to curl down toward the floor. A mallet toe often happens to the second toe, but it may happen in the other toes as well. The toe bends down at the joint closest to the tip of the toe. Causes Shoes that narrow toward the toe may make your forefoot look smaller. But they also push the smaller toes into a flexed (bent) position. The toes rub against the shoe, leading to the formation of corns and calluses, which further aggravate the condition. A higher heel forces the foot down and squishes the toes against the shoe, increasing the pressure and the bend in the toe. Eventually, the toe muscles become unable to straighten the toe, even when there is no confining shoe. 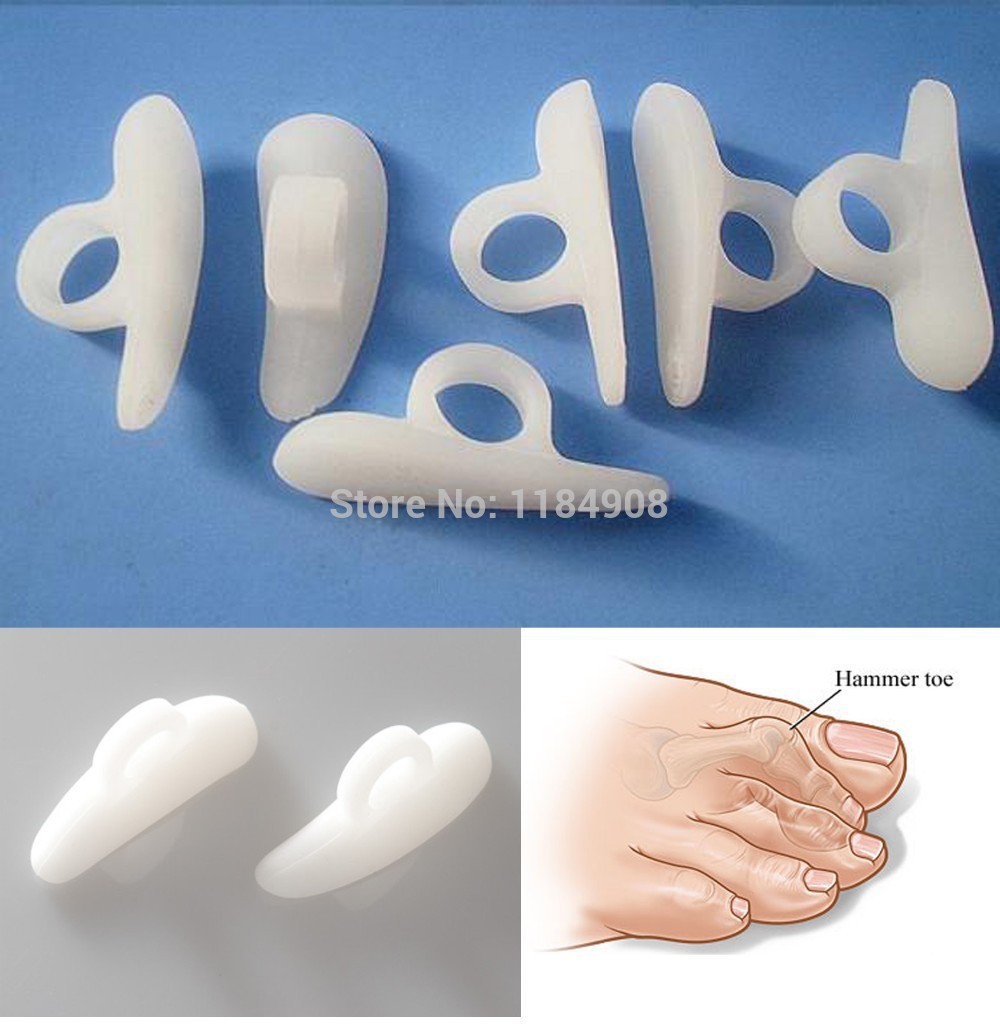 Symptoms A hammertoe causes you discomfort when you walk. It can also cause you pain when trying to stretch or move the affected toe or those around it. Hammertoe symptoms may be mild or severe. Mild Symptoms, a toe that is bent downward, corns or calluses. Severe Symptoms, difficulty walking, the inability to flex your foot or wiggle your toes, claw-like toes. See your doctor or podiatrist right away if you develop any of these symptoms. Diagnosis The treatment options vary with the type and severity of each hammer toe, although identifying the deformity early in its development is important to avoid surgery. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition. Non Surgical Treatment Non-surgical methods for hammer toes (claw toes) are aimed at decreasing symptoms (i.e., pain and/or calluses) and/or limiting the progression into a larger problem. Simple treatments patients can do are wear supportive shoes. Use an arch support. Wear shoes with a wide toe box. Modify activities. Spot stretch shoes. Periodic callus care. Surgical Treatment Surgical correction is needed to bring the toe into a corrected position and increase its function. Correction of the hammer toes is a simple outpatient surgery, with limited downtime. The best option is to fuse the deformed and contracted toe into a straight position. This limits the need for future surgery and deformity return. A new pin that absorbs in the bone or small screw is used by the Foot and Ankle Institute to avoid the need for a metal pin protruding from the toe during recovery. Although the absorbable pin is not for everyone, it is much more comfortable than the pin protruding from the end of the toe. In certain cases, a removal of a small area of bone in the deformity area will decrease pain and limit the need for a surgical waiting period that is found with fusions. Although the toe is not as stable as with a fusion, in certain cases, an arthroplasty is the best option.
Overview
 The original definition of a bunion was a bursa (a fluid-filled sac) on the side of the foot near the base of the big toe. The bursa was caused by a chronic friction of the patient's first metatarsal bone (the bone to which the big toe attaches) and the shoe. Few people go by this definition any longer. Today most people consider a bunion to be the enlarged bone on the side of the foot that typically caused the bursa. Along with this bump, there is usually an associated mis-alignment of the big toe, with it leaning in towards the second toe. In medical jargon, the term for a bunion is "Hallux Abducto Valgus," or "HAV" for short. Though the condition is really slightly different, it may also be known as "Hallux Valgus." Bunions are usually a progressive problem, and can make it difficult to find shoes that fit. The condition is often quite uncomfortable, not only because of the pressure the shoes exert on the bump, but because of the other factors associated with bunions, which we shall discuss shortly. This is usually a progressive problem, and can make it difficult to find shoes that fit. The condition is often quite uncomfortable, not only because of the pressure the shoes exert on the bump, but because of the other factors associated with bunions, which we shall discuss shortly. The original definition of a bunion was a bursa (a fluid-filled sac) on the side of the foot near the base of the big toe. The bursa was caused by a chronic friction of the patient's first metatarsal bone (the bone to which the big toe attaches) and the shoe. Few people go by this definition any longer. Today most people consider a bunion to be the enlarged bone on the side of the foot that typically caused the bursa. Along with this bump, there is usually an associated mis-alignment of the big toe, with it leaning in towards the second toe. In medical jargon, the term for a bunion is "Hallux Abducto Valgus," or "HAV" for short. Though the condition is really slightly different, it may also be known as "Hallux Valgus." Bunions are usually a progressive problem, and can make it difficult to find shoes that fit. The condition is often quite uncomfortable, not only because of the pressure the shoes exert on the bump, but because of the other factors associated with bunions, which we shall discuss shortly. This is usually a progressive problem, and can make it difficult to find shoes that fit. The condition is often quite uncomfortable, not only because of the pressure the shoes exert on the bump, but because of the other factors associated with bunions, which we shall discuss shortly.Causes Some people develop bunions from wearing shoes that do not fit correctly (especially high heels or narrow-toed shoes). For other people, bunions are caused by factors beyond their control. These can include a family history of a foot type that is susceptible to bunions, neuromuscular disorders, conditions affecting the joints (e.g., arthritis), severe injury to the foot, deformities at birth, problems that affect the way a person walks (e.g., rolling in at the ankles). Symptoms No matter what stage your bunion is in, you can be in pain. Though bunions take years to develop, you can experience pain at any stage. Some people don?t have bunion pain at all. Pain from a bunion can be severe enough to keep you from walking comfortably in normal shoes. The skin and deeper tissue around the bunion also may become swollen or inflamed. Diagnosis A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen. Non Surgical Treatment Treatment options vary with the type and severity of each bunion, although identifying the deformity early in its development is important in avoiding surgery. The primary goal of most early treatment options is to relieve pressure on the bunion and halt the progression of the joint deformity. A podiatrist may recommend these treatments. Padding and Taping, Often the first step in a treatment plan, padding the bunion minimizes pain and allows the patient to continue a normal, active life. Taping helps keep the foot in a normal position, thus reducing stress and pain. Medication, Anti-inflammatory drugs and cortisone injections are often prescribed to ease the acute pain and inflammation caused by joint deformities. Physical Therapy, Often used to provide relief of the inflammation and bunion pain. Ultrasound therapy is a popular technique for treating bunions and their associated soft tissue involvement. Orthotics, Shoe inserts may be useful in controlling foot function and may reduce symptoms and prevent worsening of the deformity.  Surgical Treatment Procedures are designed and chosen to correct a variety of pathologies that may be associated with the bunion. For instance, procedures may address some combination of removing the abnormal bony enlargement of the first metatarsal, realigning the first metatarsal bone relative to the adjacent metatarsal bone, straightening the great toe relative to the first metatarsal and adjacent toes, realigning the cartilagenous surfaces of the great toe joint, addressing arthritic changes associated with the great toe joint, repositioning the sesamoid bones beneath the first metatarsal bone, shortening, lengthening, raising, or lowering the first metatarsal bone, and correcting any abnormal bowing or misalignment within the great toe. Connecting two parallel long bones side by side by Syndesmosis Procedure. At present there are many different bunion surgeries for different effects. The age, health, lifestyle and activity level of the patient may also play a role in the choice of procedure. Traditional bunion surgery can be performed under local, spinal or general anesthetic. In the case of laser surgery, a narcotic analgesic is typically used.[5] The trend has moved strongly toward using the less invasive local anesthesia over the years. A patient can expect a 6- to 8-week recovery period during which crutches are usually required for aid in mobility. An orthopedic cast is much less common today as newer, more stable procedures and better forms of fixation (stabilizing the bone with screws and other hardware) are used. Hardware may even include absorbable pins that perform their function and are then broken down by the body over the course of months. |
